
Keratoconjunctivitis Sicca (KCS) or Dry Eye Diagnosis and Treatment
Introduction:
Keratoconjunctivitis sicca (KCS), commonly known as “dry eye,” is a most prevalent and commonly diagnosed ocular condition that affects pets, especially dogs and cats. Some breeds like Bulldogs, Lhasa apso, Pug, Shih Tzu, Cocker spaniels, West Highland White Terriers have genetic predisposition are more prone for development of KCS. KCS is less common in cats.
Literally Keratoconjunctivitis sicca means –
Kerato – Cornea, Conjunctivitis – inflammation of the conjunctiva, Sicca – dryness
It has dryness of the ocular surface and inflammation. Dryness due to lack of tear production leads to keratitis and conjunctivitis.
KCS occurs due to insufficient tear production or poor-quality tears (qualitative tear deficiency), leading to inflammation and discomfort in the eyes. Most common risk factors are aging and breed predisposition in brachycephalic dogs. In this blog post, we will explore the classification of KCS based on Schirmer’s Tear Test, discuss the signs and possible complications of each stage, and provide insights into the management strategies or treatment.
Clinical Signs and Diagnosis of KCS:
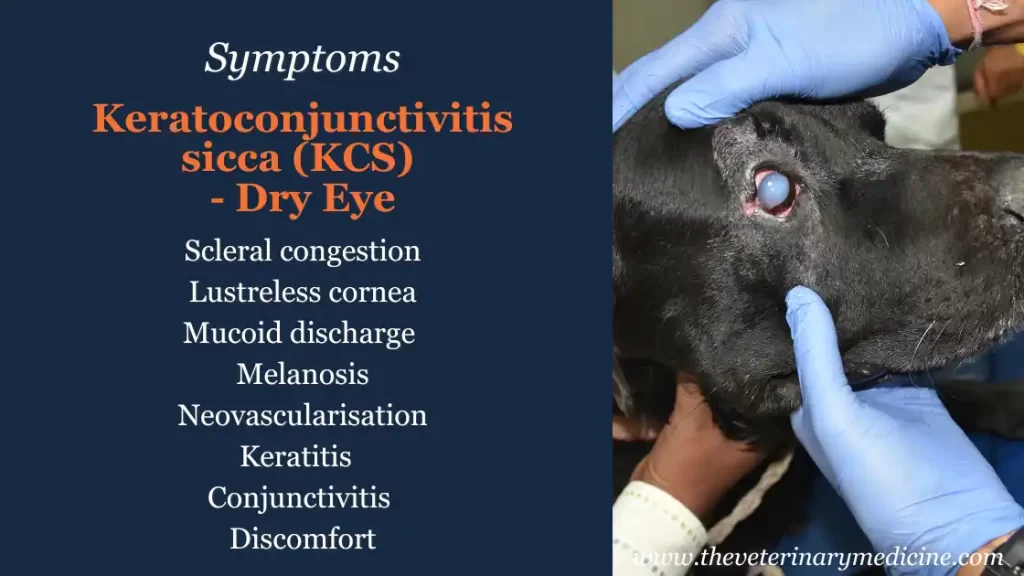
Common signs of KCS in pets include, scleral congestion (conjunctival hyperaemia), lustreless cornea, mucoid discharge, keratitis (may retain fluorescein stain and rose Bengal stain) and discomfort.
KCS is easily diagnosed with Schirmer’s tear test (STT). Tear film break up time (TBUT), Phenol red thread tear test, fluorescein dye test are additional tests which can be performed to rule out dry eye in addition to STT. Fluorescein can be used to check TBUT and dead corneal epithelial cells of dry cornea retains Rose Bengal stain which can be seen with naked eyes or ophthalmoscope. Diagnosis of KCS in cats is more difficult because of sympathetic control over tear glands.
There are two types of STT (STT-I and STT-II). STT-I is considered standard which measures basal tear production (pooled tears) and reflex tear production. STT-I is usually performed to diagnosed KCS in dogs and cats.
As tear film contains 3 parts outer-lipid, inner-mucin and center-aqueous layer and STT-I and STT-II measures only middle aqueous layer so pets with qualitative tear deficiencies (mucin and lipid) may have normal or high STT values but may show signs of ocular surface diseases like keratitis, conjunctivitis (mucin layer deficiency) and blepharitis (lipid layer deficiency).
Click Here to Read How to Perform Schirmer’s Tear Test
Classification of KCS using Schirmer's Tear Test:
Schirmer’s Tear Test is a standard diagnostic tool used by veterinarians to measure tear production in pets. It involves placing a small graduated strip of filter paper in the lower eyelid to absorb tears over a specific time (1 minute). KCS can be neurogenic (mostly due to facial nerve/ CN VII/ CN V injury), hormonal (hypothyroidism), drug induced (sulphonamides, atropine, general anaesthesia or chronic topical steroid use), post-surgical (third eye lid prolapse or cherry eye) or congenital. KCS can also be quantitative (aqueous or middle layer tear deficiency) or qualitative (mucin or lipid layer tear deficiency). Neurogenic KCS can be unilateral or bilateral according to the involvement of the nerve. Dryness due to atropine administration or anaesthesia are mostly transient. Based on the amount of tear production, KCS can be classified into four stages (most of the literature classify this only in first three symptomatic stages):
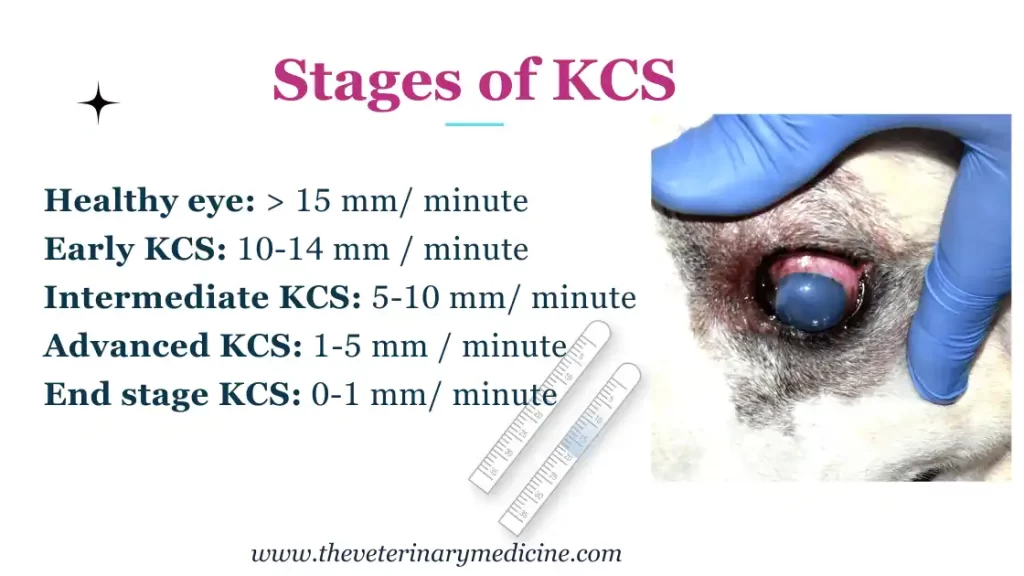
1. Stage I or Early/ Mild or Subclinical KCS:
- Schirmer’s Tear Test Result: Between 10-15mm of wetting in 60 seconds. Light reduction in tear production. Vision may not be or slightly affected.
- Signs: Mild ocular irritation, occasional squinting, and mild conjunctival redness. Symptoms are not always noticeable.
- Possible Complications: Increased susceptibility to infections. If left untreated, Stage I KCS can progress to more severe stages with prolonged inflammation, leading to potential complications.
2. Stage II or Intermediate/ Moderate KCS:
- Schirmer’s Tear Test Result: Between 5mm and 10mm of wetting in 60 seconds. In sufficient tear production.
- Signs: Moderate eye discomfort/ irritation of the eye, frequent squinting, eye discharge, conjunctival redness, and corneal changes. Loss of vision possible.
- Possible Complications: In Stage II, the lack of adequate tears may cause corneal ulceration (slower healing than usual), which can lead to pain, impaired vision, and a higher risk of frequent and recurrent secondary infections.
3. Stage III or Advanced/Severe KCS:
- Schirmer’s Tear Test Result: 1mm to 5mm of wetting in 60 seconds. Severe reduction in tear production.
- Signs: Severe ocular discomfort/ irritation, persistent squinting, marked conjunctival redness, corneal ulcers (high risk, very slow to heal and may perforate), pigmentation, corneal oedema, neovascularization, thick eye discharge and curst formation.
- Possible Complications: Stage III KCS poses a high risk of severe corneal damage, scarring, corneal perforation and potential vision loss if left untreated.
4. Stage IV or End Stage KCS:
- Schirmer’s Tear Test Result: 0 to 1 mm of wetting in 60 seconds. Severe reduction or almost no tear production. Inactive lacrimal gland.
- Signs: Very severe ocular discomfort/ irritation, persistent squinting, marked conjunctival redness, corneal ulcers (very high risk, very slow to heal and high risk of perforation), severe corneal pigmentation or melanosis, corneal surface desiccated, corneal neovascularization, thick eye discharge and curst formation. Complete and irreversible loss of vision.
- Possible Complications: Stage IV KCS poses a high risk of severe corneal damage/ perforation and permanent loss of
Management Strategies for Each Stage of KCS:
Management of KCS stages include lacrinomimetics (tear substitutes), lacrinostimulants (tear stimulants), topical antibiotics, topical anti-inflammatory drugs and surgery (PDT – parotid duct transposition) in advance or end stage.
1. Stage I KCS Management:
Treatment can resolve symptoms and treat underlying cause
- Artificial Tears: Topical lubricants and artificial tear ointments can be used to supplement the pet’s natural tear production and alleviate mild discomfort. Commonly used preparations contain hydroxypropyl methyl cellulose, carboxymethyl cellulose, hyaluronic acid, polyethylene glycol or polyvinyl alcohol.
- Anti-inflammatory Medication: In some cases, non-steroidal anti-inflammatory drugs (NSAIDs) may be prescribed to reduce ocular inflammation and discomfort. Steroidal anti-inflammatory drugs can be used for short term pain management but should not be used in eyes with ulcers or pet at high risk of corneal ulceration.
- Regular Monitoring: Regular check-ups and Schirmer’s Tear Test evaluations are essential to monitor tear production and assess disease progression.
2. Stage II KCS Management:
Treatment can stabilize the disease and prevent recurrent infections
- Cyclosporine: Topical cyclosporine eye drops help stimulate tear production and reduce inflammation. This medication is often considered the first-line treatment for Stage II KCS. Need to be administered twice daily and frequency can be increased if needed.
- Tacrolimus: In some cases, tacrolimus eye drops may be used as an alternative to cyclosporine. Tacrolimus has been proven to be more effective lacrimal stimulant in comparison to cyclosporine. Pimecrolimus (1%) has recently been demonstrated effective in KCS management when used 3 times daily.
- Antibiotics: If corneal ulcers are present, antibiotics may be prescribed to prevent or treat secondary infections. Can be used in combination with anti-inflammatory drugs like ketorolac or flurbiprofen.
- Environmental Changes: Reducing environmental factors that may exacerbate dry eye, such as exposure to smoke or dust, can be beneficial.
3. Stage III KCS Management:
Treatment partially restores sight and prevents further loss of vision.
- Topical Tear Substitutes: The use of thick artificial tear ointments or gels can help protect the cornea and provide lubrication. May have to be applied 4-6 times a day according to response. Antibiotics and anti-inflammatory medicines can be continued.
- Pilocarpine: In severe cases, pilocarpine eye drops and oral administration may be used to stimulate tear production, but its use should be closely monitored due to potential side effects. Also helpful in management of neurogenic KCS. A 0.25% topical solution can be applied every 6 hourly or 1-2% ophthalmic solution/ eye drops can be mixed with the food @1drop/10 kg body weight twice a day. Drooling, vomiting, bradycardia and diarrhoea are most commonly observed side effects in dogs due to pilocarpine administration.
- Surgical Options: In refractory cases, surgery such as parotid duct transposition or the placement of a temporary or permanent salivary duct can be considered to improve tear flow.
4. Stage IV KCS Management:
Treatment of KCS at this stage is aimed at relieving discomfort and pain. Vision cannot be saved.
- Treatment options for stage III can be followed but parotid duct transposition or the placement of a temporary or permanent salivary duct can be considered to improve tear flow. Frequent feeding to dog/ cat will stimulate salivary production which keeps lubricating the eye. May have some complications like mineral deposition on the ocular surface and infection.
Treatment of qualitative tear deficiencies depends on the source of deficiency. Blepheritis due to lipid layer deficiency can be managed by topical and systemic antibiotics, warm compress and ophthalmic ointments containing Hypromellose/ carboxy methyl cellulose.
Conjunctivitis attributed by mucin layer deficiency can be managed by using topical anti-inflammatory, antibiotics and artificial tear gels.
KCS can also develop in patients receiving sulphonamides due to cytotoxic effect on lacrimal glands.
E-collar can be put for better management and in order to precent self-mutilation. In case of painful eyes pet may not allow to instil eye drops easily and may need assistance. Orally antibiotics, anti-inflammatory drugs and vitamin A containing supplements can be added to the therapy if needed.
How to Evaluate KCS therapy:
Following changes can be noticed once you start the therapy –
- Increased STT time (may be evaluated every 3-4 weeks)
- Improved eye lid movement
- Improved patient comfort
- Improved corneal lustre and transparency
- Reduced mucus discharge
- Reduced conjunctivitis and episcleral congestion
- Slow progression of melanosis and neovascularisation
Home care for KCS affected pets:
- You can irrigate the eyes using normal/ physiological saline solution (NS), Ringer’s lactate solution (RL) or Balanced salt solution (BSS). All of these solutions are available without prescription.
- Remove excess discharge using a clean piece of cotton.
- Warm moist compress for a few minutes will help in easy removal of thick discharge.
- Keep the hairs short around the eyes and put E-Collar if pet tries to scratch.
- Monitor the eye for changes in terms of discharge and redness.
- Return for regular follow up as advised by the veterinarian.
Prognosis of KCS:
Treatment of KCS require lifelong therapy and time to time evaluation of tear production and vet checks to find out complications like neovascularization, ulceration, conjunctival congestion, infections and response to the therapy. Early and intermediate stages have good prognosis but you have to follow the medication schedule without any fail in order to prevent complications. Long term prognosis of KCS has never been favourable. Parotid duct transposition has favourable results and post operative complications like mineralization and infection can be treated symptomatically. According to a study tacrolimus 0.1% ophthalmic ointment effectively slows the progression of pigment epithelium or corneal melanosis compared to cyclosporine 0.05% eye drops. Twice daily application of tacrolimus ointment effectively stimulates tear production in dogs with KCS. Cases unresponsive to immunosuppressant (cyclosporine and tacrolimus) therapy have also been treated by injecting / topically applying allogenic canine adipose derived mesenchymal stem cells in clinical patients confirmed with KCS.
Conclusion:
Keratoconjunctivitis sicca is a common and potentially serious condition in pets, particularly dogs and cats. Early detection and appropriate management are crucial to prevent complications and preserve the pet’s vision. Regular veterinary visits, Schirmer’s Tear Test evaluations, and a tailored treatment plan based on the stage of KCS are essential for optimal care. Always consult a veterinarian for a thorough evaluation and guidance on the best course of action for your pet’s individual needs.
Check Here to Read More About:
Artificial tears / Tear substitutes: Eye Gel, VisioTears, Caneye Wet Eye Drops, Lightsense Cool Eye Drops, Opthovet Tears Eye Drops,
Tacrolimus: Tacoline Ointment, Opthocare Cool Eye Drops,
Cyclosporine: Opthocare Eye Drops, Visiocare Ointment,
Antibiotics and Anti-inflammatory Eye Drops: Ketro-Eye Eye drops, Caneye-KT Eye Drops, Opthocare KT Eye Drops,
Reference:
Christina John, Aswathy Gopinathan, Kiranjeet Singh, Pallvi Sharma and Chelladurai Sowbharenya. (2018). Clinical evaluation of topical tacrolimus ointment usage in different stages of keratoconjunctivitis sicca in dogs. Turkish Journal of Veterinary & Animal Sciences. Vol. 42: No. 4, Article 5. PP 259-268.
Wei, LN., Wu, CH., Lin, CT. et al. Topical applications of allogeneic adipose-derived mesenchymal stem cells ameliorate the canine keratoconjunctivitis sicca. BMC Vet Res 18, 217 (2022). https://doi.org/10.1186/s12917-022-03303-7
Dodi PL. Immune-mediated keratoconjunctivitis sicca in dogs: current perspectives on management. Vet Med (Auckl). 2015 Oct 30;6:341-347. doi: 10.2147/VMRR.S66705. PMID: 30101119; PMCID: PMC6067592.
Disclaimer: Self-medication of your pet without vets recommendation may result into loss of the eye or life threatening in case of pilocarpine like medicine side effects.


